
Male Sexual Disorders
SEXUAL DYSFUNCTIONS IN MALE:
SEXUAL DESIRE DISORDERS :
- Hypoactive sexual desire disorder
- Sexual aversion/ inhibition Syndrome
- Hyperactive sexual desire disorder (?)
2) SEXUAL AROUSAL DISORDER :
- Male erectile disorder (Impotence)
3) SEXUAL ORGASMIC DISORDER
- Inhibited (absent) Male orgasm
- Male Premature orgasm (Early Orgasm Disorder)
4) PAINFUL SEXUAL SYNDROME
- Male Dyspareunia
LOW or ABSENCE OF SEXUAL DESIRE
Persistently or recurrently deficient (or absent) sexual fantasies and desire for the sexual activity. It causes marked distress or interpersonal difficulty amongst the partners.
Sexual desire is expressed in sexual dreams, fantasies, attraction to erotic material, wish for sexual activity etc.
Men having low/absent sexual desire have low/absent interest in initiating any sexual behaviors and do not respond to partner’s sexual urges.
Any individual’s sexual urge may not remain same throughout the life. It may have natural ups and down. It also changes in relation to one’s age, nature of upbringing, current relationship and other situational factors.
Causes:
I. Organic : any condition which causes disturbances in hormones esp. low level of Testosterone hormone, Low level of thyroid hormone and high level of Prolactin in blood may lead to low sex desire. Pituitary Diseases and Primary Testicular Diseases are mainly responsible.
Systemic diseases that causes testicular disorders… like Chronic Renal Failure, Cirrhosis, Cushing’s Syndrome, Estrogen producing Tumors, Hypothyroidism, Diabetes Mellitus, Stroke, Parkinson’s Disease and certain Medicines can also cause this situation
II. Psychogenic : Anger, fear & distraction etc can act as ‘turn off’ mechanism. Some factors cause negative thoughts. Guilt about sex, anticipation of lack of pleasure, Emotional distress, Depression, Interpersonal conflicts between the partners, hostility, lack of trust, rejection etc. can also reduces sex drive.
Physical Examination :
A thorough general and local examination needs to be performed.
General examination includes parameters like Blood Pressure etc.
Local examination is done to recognise the genitals for the congenital deformities, presence of infection, trauma, personal hygiene etc.
Laboratory Investigations :
General investigations like Blood Sugar, Lipids, Liver function tests, Kidney function tests etc. should be performed to identify underlying causes.
Hormonal assay like Testosterone, FSH, LH, Prolactin may be necessary.
Treatment :
Counselling and Psychosexual Therapy is the main backbone of the treatment. Couple marital Counselling and sexuality education may be necessary for the problems when both the partners have relationship problems. Behavioural therapy helps to reduce performance anxiety. The main aim of the therapy is to remove guilt and fears blocking the natural sexual response.
Medicines like hormonal supplements may be necessary in some cases.
Sex Tonics (Aphrodisiacs) : It is a common belief that certain substances like Ginseng, Rhino horn powder, Tiger’s bones, Food substances like Onion, Garlic can enhance the sexual desire. But, there is no drug or food substance that increases the sexual power
ERECTILE DYSFUNCTIONS : ED (IMPOTENCE)
Persistent or recurrent inability to attain, or to maintain an adequate erection, until completion of the sexual activity.
The disturbance causes marked distress or interpersonal difficulty.
Although an erection may not be an absolute requirement to prove a man’s potency, it is considered by many men and women as the clear sign of men’s strength, virility and sexual identity. This is why ED evokes feeling of embarrassment, shame, anxiety and incompleteness in a man.
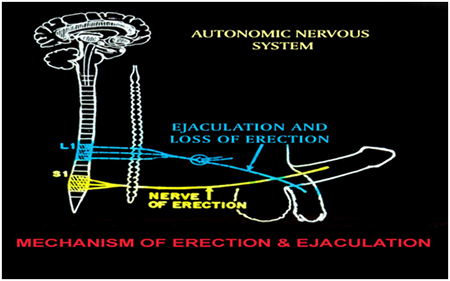
How erection takes place
The mechanism of erection is a complex mechanism. It takes place when the blood flow increases and swells the spongy tissues of the penis triggered by physical or psychological stimulations.
The ‘sex center’ in the brain receives the sensory inputs from all five special senses – touch, sight, hearing, smell and taste – play an important role in sexual arousal.
Sexual responses are largely controlled by Autonomic Nervous System (ANS) which is not under will power. Erection just happens when one is sexually turned on.
- Parasympathetic nervous system is responsible for the erection in males and lubrication in females. On receiving stimulations, the sex cnter in brain transmits the messages to muscles and blood vessels which relaxes and allows more blood to flow to fill up the spongy tissues of the penis causing ‘Erection of the Penis’. The veins have valves which prevents the blood from leaving penis thus sustaining the erection.
- Sympathetic nervous system is responsible for ejaculation and loss of erection.
There are many neurotransmitters and molecules required to bring about the process of erection.
Causes of ED :
I. Psychosocial :
Ignorance about sex, Fear of failure, Lack of communication, disturbed relationship, Guilt about sex, low self esteem, religious restrictions, Oedipus complex, numerous myths and misconceptions causing performance anxiety.
Many men have un-realistic expectations about the onset, rigidity, duration and frequency of erection.
Negative feelings towards partner (like disliking, hostility, lack of interest etc) can also cause difficulty in erection when the sex in attempted.
Just like a person can not sweat according to his own wish, similarly a man can not develop erection according to his own wish. Erection occurs as a result of sexual excitement.
II. Functional :
Stress, Boredom, Fatigue, Anxiety, Depression etc. can also cause less excitement and a s result ED may occur.
Isolated / single episodes of not having an erection or loosing the one at some stage of the life is a common occurrence in men’s life. They are the temporary form of response to stress, lack of privacy etc. any event (like putting on condom) that puts break in the continuity of the excitement can lead to self consciousness resulting into loss of erection.
Fear of sexual performance is also likely to dampen the sexual arousal and loss of erection. On long term basis, performance fears may lead to loss of self esteem, lowered interest in sex. Both partners may become the ‘spectators’ during sex by observing and evaluating their own performances rather than finding pleasure from each other.
III. Organic :
2. Metabolic: Diabetes Mellitus is the major cause for ED. It causes narrowness of the blood vessels thus reduces blood flow to the penis. Also it causes weakness in the nerves. Both these are responsible for ED
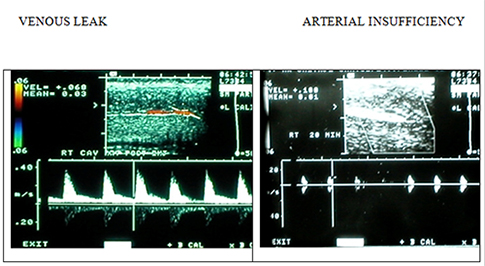
3. Vascular : Hypertension also reduces elasticity of the blood vessels. So, blood flow to the penis reduces causing ED. Congenital arterial dysplasia causes ED by birth
Venous leakage causes loss of erection before completing the act.
4. Neurogenic : Spinal Cord injury, Peripheral Nerve diseases reduces the sensory flow. So, the impulse from brain does not reach penis blood vessels causing ED
IV. Drugs :
Anti-diabetec, Anti-hypertensives, Psychotropic medicines and variety of other medicines when taken for long duration have serious side effects in the process of erection by disrupting the neurotransmitters.
Physical Examination :
A thorough general and local examination is performed.
General examination includes parameters like Blood Pressure etc.
Local examination should include the genitals for the congenital deformities, presence of infection, trauma, personal hygiene etc.
Laboratory Investigations :
General investigations like Blood Sugar, Lipids, Liver function tests, Kidney function tests etc. should be performed to identify underlying causes.
Hormonal assay like Testosterone, FSH, LH, Prolactin may be necessary.
The ultimate goal of the investigations is to determine the causative factors for diagnosis, prognosis and management of the dysfunction.
I. EVALUATION OF VASCULAR SYSTEM :
1. Peno-Brachial Index : here the blood pressure of the penis and the arm is measured and compared. Large difference between these two readings suggests compromised penis blood supply.
2. Intracavernous Injection test : The injection of a smooth muscle relaxant like Papaverine or Prostaglandin, directly into one of the corpora cavernosa normally creates a rigid erection. The medicine relaxes the smooth muscles of corpora and dilates the blood vessels.

Failure of the injection to produce erection even after sufficient dose is suggestive of vascular erectile dysfunction. Then more sophisticated tests may be needed.
It is one of the simple office procedure that gives the working diagnosis in about 70% of the cases.
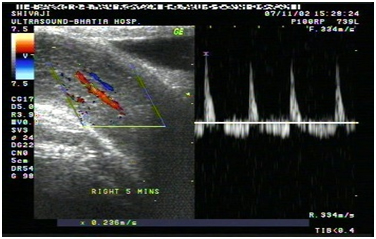
A Doppler study can be easily combined with the injection test. If an objective measurement of the erection is desired either for academic, medico-legal or psychotherapeutic purposes, a real time Rigiscan monitoring may be performed in the same session.
3. Duplex Ultrasonography : Ultrasonographic evaluation of the cavernosal arteries can be performed once cavernosal smooth muscles has been relaxed by vasoactive drug. This helps visualization of the cavernosal arteries and the measurement of the flow and the venous drainage too.
4. Dynamic Infusion Cavernosometry and Cavernosography (DICC): this test evaluates both arterial and venous systems i.e. corporal veno-occlusive dysfunction. Technique involves precise measurements of the fluid pressure changes within the penis during erection.
PENILE DOPPLER : USG mode
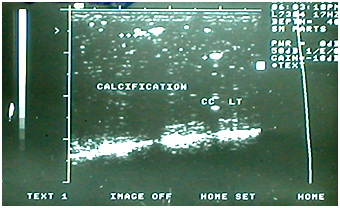
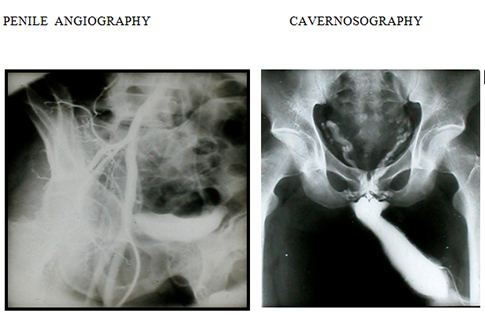
5. Arteriography and Cavernosography (Vascular X-rays) : These X-rays can demonstrate disorders inside the penis such as scar tissue, arterial blockage, venous leakage and abnormal vascularity.
Indicated only when a definitive vascular diagnosis is needed or when vascular reconstructive surgery is being considered.
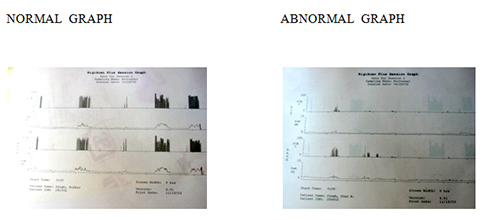
II. EVALUATION OF NOCTURNAL ERECTIONS:
A healthy male has two-four episodes of erection during night sleep. A person having functional Erectile Dysfunction will continue to have these erections whereas organic Erectile Dysfunction will show absence of such erections.
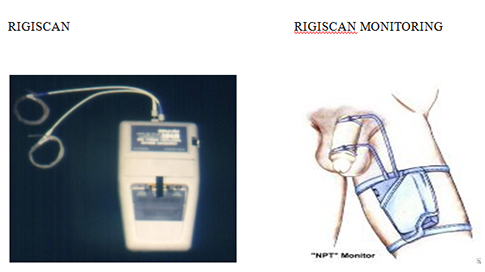
These erections are measured and recorded by Nocturnal Penile Tumescence and Rigidity (NPTR)- Rigiscan monitoring. The small electronic Rigiscan monitor is strapped to the thigh. The monitor is attached to the special loop that are placed around the penis. The patient goes to sleep with monitor on throughout the night.
The Rigiscan monitoring provides a thorough and reliable report of all night-time penile activity. The frequency, quality, duration and amplitude of night time erections can be accurately determined.
III. EVALUATION OF NEUROLOGIC FUNCTION :
These include Nerve conduction studies, Biothesiometry and Corpus Cavernosum Electromyography (CCEMG). Not so frequently used as they are not so reliable. Diagnosis of neurogenic E.D. is based on high index of clinical suspicion, thorough neurological examination and elimination of vasculogenic causes.
Treatment of Erectile Dysfunction
Counselling and Psychosexual Therapy is the main backbone of the treatment.
Couple marital Counselling may be necessary for the problems when both the partners have relationship problems.
There are specific therapies like SENSATE FOCUS therapy etc.
1. Oral Medications :
Sildenafil (Viagra), Tadalafil (Cialis) and Vardenafil (Levitra) are the drugs from this group which are commonly used.
It must be remembered that if the man is not sexually stimulated, erection will NOT result.
They are not useful in cases of Early ejaculations as they don’t alter the ejaculatory reflex.
Since PDE inhibitors are present in other tissues of the body mainly retina and myocardium, they do produce certain unwanted adverse reactions. There are specific indications and contraindications to these drugs which must be followed strictly.
1. Yohimbin, Delequamine, Fluparoxan, Idazoxan, Phentolamine etc are drugs with variable efficacy.
Antidepressants : Certain atypical Selective Serotonin Reuptake Inhibitors (SSRI) are believed to be helpful as they are 5-HT agonists. Trazodone, Fluoxatine etc are commonly used drugs.
1. Dopamine Agonists : Apomorphine was commonly used drug.
2. Nitric Oxide (NO) donors : Linsidomine (SINE1), Sodium Nitroprusside etc.
2. Intra Penile Injections : When vasodilatory drugs like Papaverine, Phentolamine, Chlorpromazine and Prostaglandine E1 etc alone or in combination are injected into the corpora cavernosa of Penis, they act directly on the penile arteries and cavernosal smooth muscles bypassing the psychological, neurological and hormonal systems to provide an erection equals to the individual’s vascular capacity.
The principle is outlined while describing Diagnostic ICIVAD.
ICIVAD produces good erection in 70-80% of men.
These men learn to self inject themselves at home and have intercourse.
Indicated for short term in cases (which are not responding to other modes of treatment due to high anxiety etc). until they regain their confidence. Whereas Neurogenic and Vasculogenic cases may require long term therapy.

Possible immediate complications are local pain, haematoma formation and Priapism (Prolonged and painful erction). While fibrosis in penis is a late complication. Both complications can be minimized.
PRIAPISM (Prolonged and painful) is one of the important complication which takes place, if the dose exceeds the required dose and as a result penis remains erect for many hours. It should not be ignored. However, it can be treated easily if person comes within 6 hrs of prolonged erection. A person should avoid using self injections if he does not have facility to reduce priapism (if it developes)
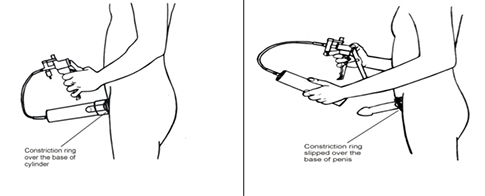
2. Vacuum Erection Device : A Vacuum Device consists of a hollow cylinder attached to a pump. The penis is placed within the cylinder and the mouth of the cylinder is pressed against pubic fat. When activated, the pump creates vacuum in the cylinder i.e. around the penis. As a result, due to negative suction pressure, blood rushes into the penis. A ring is then placed around the base of penis to retain the erection.
Very much suitable for men having vascular and neurogenic Erectile Dysfunction.
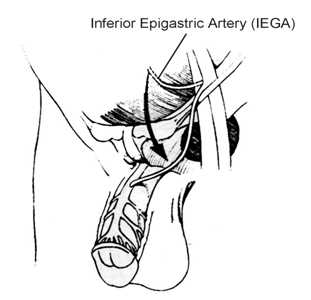
3. Surgery : 2 types of surgeries are available for erectile dysfunction
(1) Penile Revascularisation : Involves either ligation of penile veins ( to reduce the venous drainage) in cases of Vaso-occlusive disorders OR anastomosis of the inferior epigastric artery to the penile vessels ( to enhance the arterial flow).
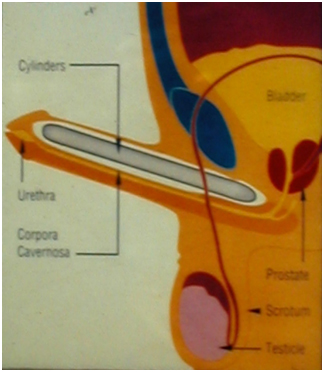
(2) Penile Prosthesis Implantation : Penile Prosthesis are a mechanical devices which are permanently implanted into the corpora cavernosa of penis to render it rigid enough for intercourse.
Earlier attempts were done as early as 1936 where rib cartilage was used to stiffen the penis. Now, silicon implants are used with which artificial erections can be achieved which closely resemble the natural erections
Two types of Penile Implants are available.
a) Inflatable : Here the cylinders of the implants are hollow and are connected to the reservoir. When required, fluid can be made flow through valve, into the cylinders thus causing them to erect.
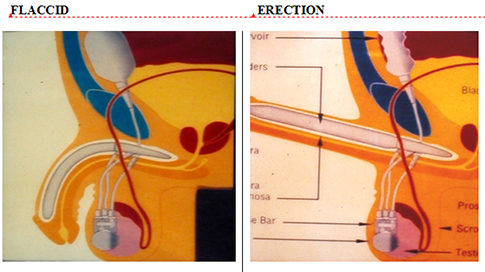
b) Non-Inflatable (Rigid) : Here the cylinders are rigid having constant girth thus rendering permanent erection. But the hinge allows bending of the prosthesis making concealment easy for the person.
PREMATURE EJACULATION (EARLY ORGASMIC RESPONSE)
Persistent or recurrent ejaculation with minimum sexual stimulation before, on, or shortly after penetration and before the person wishes it.
It is also known as early ejaculatory disorder.
It has been difficult to quantify the duration of ejaculation because there is no such thing like standard ejaculation. The duration of ejaculation largely varies from person to person and in the same person too, it varies a lot depending upon the situation, partner and level of excitement.
Gaining control over ejaculation is a learning process and can be taught easily when a person indulges into sex frequently.
Early ejaculation is common in the initial days of marriage, after long period of absence, absence of privacy, performance pressure etc……
Female partner’s estimate of duration of time can be misleading.
Many young men misinterpret the urethral gland’s secretion as semen and become un-necessarily worried about it and may lose sleep and peace over the imaginary disease.
Many men do have an un-realistic expectation about the duration of the sexual intercourse after watching pornographic films or listening to some of his friend’s experience.
Whereas some men consider themselves as premature ejaculators because their partners never experience climax during intercourse.
This disorder can affect the sexual satisfaction level of one or both partner and can create significant stress amongst them.
Grading Severity of Premature ejaculation :
- Grade I : Ejaculation Before Vaginal Insertion
- Grade II : Ejaculation On or just after vaginal Insertion
- Grade III : Ejaculation after some thrusting.
There are 2 classes of premature ejaculation
I : Situational : Occurring in some specific situation like new place, partner or intercourse after prolonged abstinence.
II : Global : Occurring in all the situations irrespective of other factors.
CAUSES of PREMATURE EJACULATION :
- 1. Situational : in a particular situation due to various reasons like.. Anxiety, Fear of losing erection, Hurried Sexual experience, fear of being caught, in sufficient privacy, prolonged sexual abstinence, excessive sensitivity of penis tip etc…
- 2. Constitutional : some men have ‘low threshold’ for ejaculation which means their sexual excitement bearing capacity is very low. With minimum sexual excitement, their excitement increases very rapidly and immediately they experience climax and ejaculate very quickly.
Treatment of Premature Ejaculation
Counselling : thorough understanding of the problem by the person and his partner is essential.
Man often feels frustrated, dejected, helpless and may consider him good for nothing. This feeling of being ‘incomplete’ may be so intense that it affects his other functioning and routine activities too. Fear of embarrassing situation and humiliation may result into avoidance of sexual activities.
His partner may find it hard to understand his problem. She may also feel frustrated, angry, unsatisfied and critic of his man and may become non co-operative.
For successful outcome, couple needs motivation, understanding and perseverance.
Sex therapy for premature ejaculation:
Ejaculatory control is a learning process.
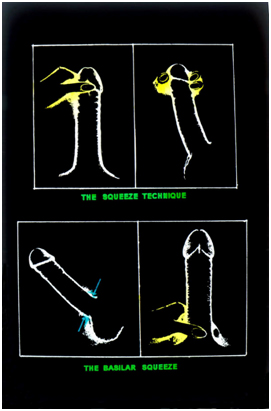
In order to learn ejaculatory control, the following sequence of exercises are effective. Two techniques have been developed – “stop-start” or “squeeze” technique.
The basic principle is to increase the awareness of sensations of ‘point of no return.’
Procedure :
1.• When alone :
In this one masturbates and before reaching the stage of “no return’, stops and allows the arousal to decline and then starts again. This can be continued for about 15 min. the pause should be long enough so that the stage of inevitable ejaculation doesn’t follow immediately after starting.
2.• With Partner :
Here the partner helps the man to identify ‘point of no return’. She helps man masturbate to reach that point where man tells her to stop before inevitable orgasm. Then adequate pause is necessary to allow arousal level subside slightly. This is repeated for about 15 min.
Now they are ready for Sensate focus therapy. They proceed as mentioned above. Once the anxiety level begins to fall and confidence builds up, ability to control ejaculation improves steadily.
Alternately, “SQUEEZE” method can also be used. Here, just before the point of no return, one stops the stimulation of the penis and then man or his partner grasps the tip of the penis between fingers and thumb at the attachment of foreskin near coronal sulcus for about 10 seconds. This reduces the reflex ejaculatory response. Then the stimulations are resumed and the procedure is repeated as per necessity.
Although sex therapy offers no instant, magical cures, many studies have shown that it is of significant help to many couples. The outcome depends upon the readiness of the couple and efforts of the therapist. Hence there are variations in the results.
Medical Treatment of Premature ejaculation
There are various medications available in the market for delaying the ejaculation. Medication delays ejaculation through neuronal route.
Most of the herbal / ayurvedic medications are found to be non effective because they are prescribed in a general manner. Ayurved is a science that treats disease according to the constitution (prakruti) of the person. A medicine that is useful to one person may be totally ineffective to other person because of different constitutions.
Modern medicine (Allopathy) uses medications that are primarily prescribed for depression (Anti-depressant medication). Fluoxetine, paroxetine, Sertaraline, etc are commonly prescribed with beneficial effect.
Remember, that medication can not cure the problem permanently. It will delay the ejaculation as long a person takes it. During this treatment period person should develop control through the behavioral techniques like “stop-start” and “squeeze” methods.
DELAYED / ABSENT EJACULATION
Persistent or recurrent delay in or, absence of, orgasm following a normal sexual excitement phase during sexual activity.
It is also known as Inhibited male orgasm, Absent Orgasmic Response or Anejaculation.
In this disorder, a man can not reach climax during sexual intercourse although he can ejaculate by manual or oral stimulation. Some men reach climax but only after very intensified stimulation, some can ejaculate only during masturbation. These men have ejaculation during sleep (night fall)
Causes : Mostly situational.commonle seen in situations like - Inability to give semen sample in lab. for examination. They find it difficult to fantasy during masturbation to collect semen sample in laboratory.
Many persons have high threshold for reaching orgasm i.e. they require high and persistent sexual stimulations to reach to orgasm. They may not reach climax and hence do not ejaculate. Often they have involuntary ejaculation during sleep.
Some men have various functional reasons. They somehow lack the sexual fantasy and conditioning. They often fail to register sexual pleasure during intimacy. Rather, their sex act becomes very mechanical without any sensation.
Dislike for partner, masturbation guilt, religious restrictions, fear of pregnancy etc are some of the common reasons for which a man may be inhibited and sub-consciously, avoids ejaculation.
Often presents as Primary Infertility as failure to deposit semen in the vagina causes failure in conception.
Treatment:
Sex therapy – Sensate focus therapy may be helpful.
Vibrator: vibrator provides strong, prolonged penile stimulation. When applied over the penis, the strong stimulations help the person to reach orgasm. Sometimes it may take up to 2-3 hrs to ejaculate. Regular and repeat use of vibrator reduces the time to reach climax.
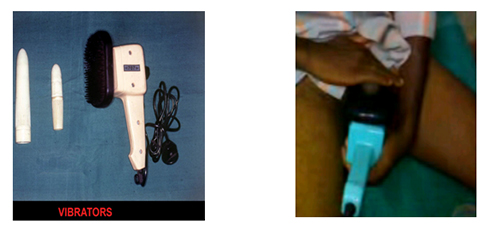
For Fertility, vibrators are of great help..
- 1) in the laboratory while giving semen sample for semen analysis.
- 2) during artificial insemination, intra-uterine-insemination (IUI) or even in In-Vitro-Fertilization (IVF – test tube baby procedure)
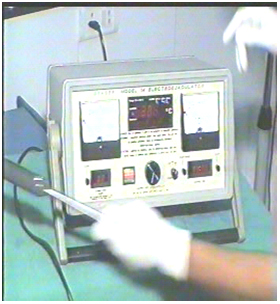
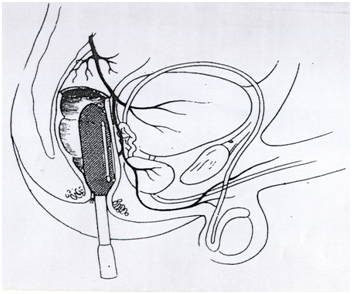
In the cases who do not respond to Vibrator Therapy, Electro-Ejaculation Therapy is indicated. In this technique, seminal emission and ejaculation is induced by direct electrical stimulation of the efferent nerves innervating the seminal vesicles and the terminal vas. The procedure is carried out using Electro-ejaculator which delivers current of 0-1 amp at 0-50 volts. It requires general anesthesia.
PAINFUL SEX (DYSPAREUNIA)
Recurrent and persistent genital pain associated with sexual intercourse in male.
The disturbance causes marked distress or interpersonal difficulty.
The pain may occur on erection of penis or on insertion and thrusting or after ejaculation
Causes :
- • Pain on erection : Infection, Trauma, Phimosis (tight foreskin of penis), chordee (curvature in penis) etc.
- • Pain on Insertion : Inadequate lubrication, wrong direction, trauma, chemical irritation etc.
- • Pain after ejaculation : Urinary infection or calculus in urinary tract.
Humour in sex



